 Français
Français Español
Español Products
Products

 About Us
About Us







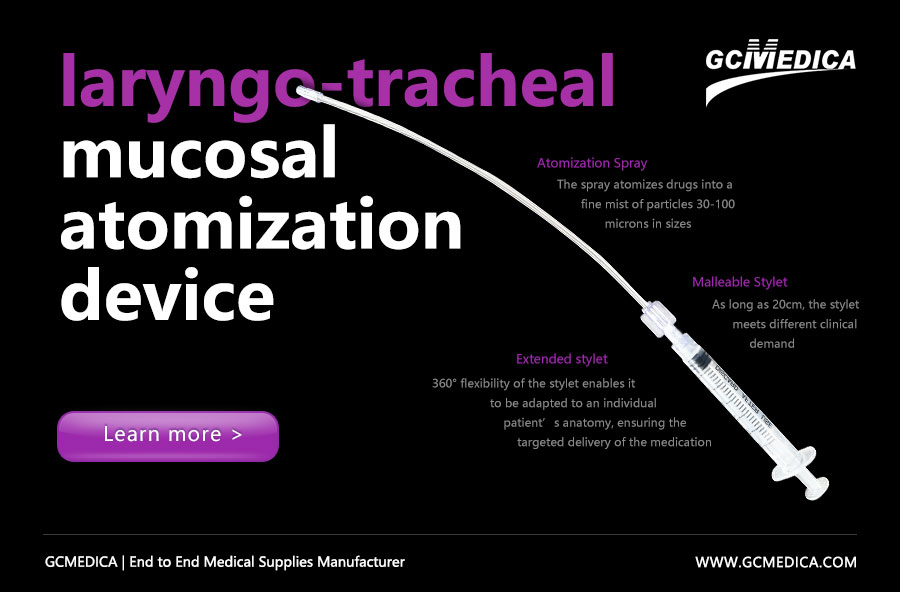
In settings where topical anesthesia and humidification of the laryngo-tracheal mucosa are required—such as awake fiberoptic intubation, bronchoscopy, or management of airway hyperreactivity—the Laryngo-Tracheal Mucosal Atomizer (LTMA) offers a simple, reproducible means to deliver fine, evenly distributed aerosolized medication. Its gentle, low-pressure spray minimizes coughing and patient discomfort while maximizing surface coverage of lidocaine or other local anesthetics. Proper preparation, device handling, and patient positioning are crucial to achieve optimal mucosal absorption and to reduce procedural risks.
Prior to use, confirm that all components of the LTMA kit—syringe adapter, atomizing nozzle, connecting tubing, and sterile syringes—are intact and free of obstruction. Draw up the prescribed concentration of topical agent (commonly 2–4 mL of 2% lidocaine) into a 10 mL syringe, ensuring no air bubbles are present. Secure the syringe to the adapter, then attach the atomizing tip, holding it firmly to prevent leakage under slight positive pressure. With the patient’s head extended in a “sniffing” position and mouth partially open, gently advance the nozzle into the oropharynx just above the glottic inlet. Depress the plunger at a steady rate, creating a fine mist that coats the supraglottic structures. For subglottic application, advance the nozzle tip through the vocal cords under direct visualization or fiberoptic guidance, and atomize as you withdraw. Monitor the patient for signs of systemic toxicity—especially if cumulative doses exceed 7 mg/kg of lidocaine—and provide supplemental oxygen if needed.
The following table summarizes the major steps, recommended volumes, and practical considerations:
| Step | Action & Volume | Key Points |
|---|---|---|
| 1. Preparation | 2–4 mL of 2% lidocaine in 10 mL syringe | Remove air bubbles; confirm device integrity. |
| 2. Assembly | Attach syringe → adapter → atomizer tip | Ensure snug connections; avoid leaks. |
| 3. Patient Positioning | “Sniffing” head extension; mouth open ~2 cm | Aids direct spray path; reduces gag reflex. |
| 4. Supraglottic Atomize | Advance tip to oropharynx; spray 0.5 mL/sec | Maintain steady plunger pressure. |
| 5. Subglottic Atomize | Under visualization, pass tip beyond cords | Spray while withdrawing nozzle gradually. |
| 6. Monitoring | Observe for cough, dysphonia, toxicity | Total lidocaine ≤7 mg/kg; have resuscitation ready. |
By following these structured steps and utilizing consistent spray technique, clinicians can achieve reliable mucosal anesthesia with minimal patient discomfort and reduced procedural complications.